Duodenal Perforation Presenting as Acute Appendicitis (Valentino Syndrome) in a Resource Limited Setting: A Case Report
Authors
Keywords:
- Valentino syndrome, duodenal perforation, acute appendicitis mimic, modified Graham patch.
Abstract
Background: Right lower abdominal pain is a frequent emergency presentation with varied differential diagnoses. Valentino syndrome describes a perforated gastric or duodenal ulcer presenting as acute appendicitis due to tracking of gastrointestinal contents to the right iliac fossa.
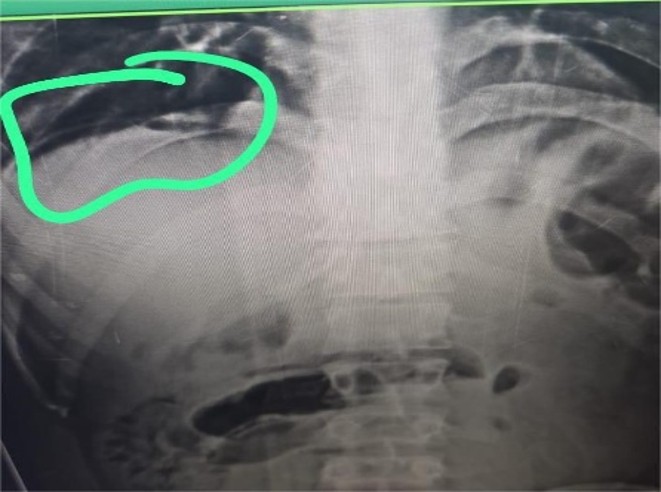
Case Summary: A 28-year-old male presented with obstipation, non-bilious vomiting and acute lower abdominal pain. Examination showed tachycardia, tachypnoea and diffuse abdominal tenderness with guarding. Plain radiograph revealed pneumoperitoneum. Exploratory laparotomy revealed an inflamed appendix with purulent collection in the right iliac fossa, for which appendicectomy was performed. Further exploration identified a perforation at the junction of the first and second parts of the duodenum, which was repaired with a modified Graham patch. The postoperative course was uneventful.
Conclusion: Valentino syndrome should be considered in patients presenting with right lower abdominal pain, especially in resource-limited settings where advanced imaging is not readily available. Thorough intra-operative assessment is essential for correct diagnosis and management.
Downloads
References
1. Pearson FG (1949) Valentino’s syndrome: Acute right iliac fossa pain due to perforated peptic ulcer. Am J Surg 77: 342-344.
2. Hsu SY, Huang SP, Hsu WH, Yu JC (2005) Perforated peptic ulcer presenting as acute appendicitis (Valentino’s syndrome): Case report and literature review. World J Gastroenterol 11: 1767-1769.
3. Levenson RB, Smith BB, Novelline RA (2008) Right lower quadrant pain: Imaging diagnosis and differential considerations. Radiographics 28: 1019-1036.
4. Sadeghi R, Ilyas M, Richardson JD (2013) Evaluation and management of perforated peptic ulcer disease in resource-limited settings. Surg Clin North Am 93: 1273-1290.
5. Puri V, Saini S, Gupta P (2017) Peptic ulcer perforation: evolving role of imaging and laparoscopy in diagnosis and management. Indian J Surg 79: S30-S38.